Introduce yourself, confirm the patient's name and date of birth. Explain the purpose of the examination, and obtain consent. Ask the examiner to act as a chaperone and then proceed to wash hands. Adjust the bed to a 45° angle.
General inspection
Begin the examination by inspecting the patient. The patient should be exposed from the waist up. Offer a blanket to maintain the patient's dignity and inform women that they may keep their undergarments on. Ask the patient to expose their legs as well, as there may be some obvious peripheral oedema.
Ask the patient if they are in any pain and are comfortable. Observe for any obvious scars. Ask the patient to cough as this may reveal an incisional hernia. Check the skin colour for any pallor (anaemia), jaundice or hyperpigmentation (haemochromatosis). Be sure to also assess the age of the patient and their hydration status. Note any paraphernalia around the bedside, looking for clues such as a stoma bag or catheter.
Two important causes of anaemia are iron malabsorption and blood loss. The presence of anaemia needs to be promptly addressed.
Causes of jaundice can be split into pre-hepatic, hepatic and obstructive:
Pre-hepatic jaundice: Hyperbilirubinaemia secondary to is described when there is an increased production of bilirubin or decreased uptake by hepatocytes. There will be a large amount of unconjugated bilirubin in the blood.
Hepatic jaundice: Hyperbilirubinaemia due to a failure of the liver to metabolise or excrete the bilirubin efficiently enough. There will be an increase in both conjugated and unconjugated bilirubin in the blood.
Post-hepatic jaundice: Hyperbilirubinaemia secondary to stasis of the biliary system (for example, gallstone obstruction). Conjugated bilirubin is unable to flow from the liver to the gut. It can be hepatocellular or biliary in nature and will result in a build-up of conjugated bilirubin in the blood. As bilirubin is unable to reach the gut, the stool will develop a pale colour. Instead the conjugated bilirubin will be excreted via the kidneys and the patient's urine will turn dark.
Hands
Inspection of the hands should be done in an intentional and noticeable way. Look at the nails carefully for the following signs:
Clubbing: This can be due to inflammatory bowel disease, coeliac disease, GI lymphoma or malabsorption.
Koilonychia (curved, spoon-shaped nails): Koilonychia can be a result of iron deficiency or in rarer cases secondary to haemorrhage.
Leukonychia (white patches on nails): Leukonychia can be due to hypoalbuminaemia. Hypoalbuminaemia may be present in liver cirrhosis and certain renal pathologies (i.e. those which result in nephrotic syndrome).
Muehrcke's lines (leukonychia striata, or leukonychia extending across the nails): Can also be due to hypoalbuminaemia.
Check the palms for pallor (anaemia), erythema and Dupuytren's contracture (alcoholism).
Ask the patient to hold their hands outstretched, cock their hands back at the wrist joint and hold that position for 30 seconds. This checks for asterixis, where the wrists will begin to flap as a result of hepatic encephalopathy.
Dupuytren's contracture is a result of palmar fibromatosis, and it can be a relatively non-specific sign. It may be familial or due to a large number of pathologies including alcoholism
Check the arms for excoriations (scratch marks). This can be a result of bile salt accumulation in the skin in obstructive jaundice. Look out for needle track marks too; intravenous drug use is an important risk factor for viral hepatitis. Finally check for bruising, as liver disease can result in reduced clotting.
Check the radial pulse, assessing rate and rhythm. Offer to measure the patient's blood pressure.
Face
Inspect the eyes for pallor (due to anaemia, best viewed on the lower aspect of the sclera) or icterus (i.e. jaundice, best viewed on the superior aspect of the sclera). Corneal arcus (blue/grey ring in the in the periphery of the iris) may be present in dyslipidaemia and Kayser–Fleischer rings (brown/grey rings in the in the periphery of the iris, formed by copper deposits) may be present in Wilson's disease (hepatolenticular degeneration). Uveitis (inflammation of the iris, ciliary body and/or choroid), may present with eye redness and photophobia, and can arise present in patients with inflammatory bowel disease.
Check the cheeks for a malar rash, a sign of systemic lupus erythematosus. Ask the patient to open their mouths and check for:
Aphthous ulcers: These are benign, non-contagious mouth ulcers which can occur in inflammatory bowel disease.
Macroglossia (large tongue): This can occur in vitamin B12 deficiency.
Glossitis (inflammation of the tongue): There are multiple causes of glossitis including vitamin (B) and mineral (iron) deficiencies, infection, Crohn’s disease and many more. Types include atrophic glossitis and strawberry tongue.
Angular cheilitis (cracked lip corners): Caused by iron deficiency anaemia or B12/folate deficiency.
Brown freckles: This may be a sign of Peutz-Jeghers syndrome, a disease in which many benign polyps develop in the GI tract.
Oral candiadasis: This is a result of a Candida albicans infection and can occur in HIV infected patients or those with diabetes mellitus.
Patients may sometimes appear to have yellow eyes, but not have jaundice. This is particularly prevelant in patients who live/have lived in hot countries for extended periods of time, as the yellowing is an effect of the sun, rather than bilirubin levels. To be sure, lifting the patient's upper eyelid will reveal true jaundice.
Glossitis refers of inflammation of the tongue. This can be infective or nutritional in origin. The tongue will be sore, the dorsal surface will usually be smooth and erythematous, and there will be absence of some of the lingual papillae. Two important types of glossitis are as follows:
Atrophic glossitis: A depapillated, glossy and tender tongue usually caused by an iron deficiency anaemia or due to a vitamin B12 deficiency.
Strawberry tongue: An erythematous tongue with relatively enlarged fungiform papillae. Causes include scarlet fever and Kawasaki disease.
Palpate the left supraclavicular fossa for Virchow's node. This lymph node is a common site of metastasis for gastric cancer.
Chest
Inspect the chest for spider naevi, which can be due to increased oestrogen levels in alcoholic or hepatitic cirrhosis. Spider naevi can indeed be idiopathic, yet more than five is almost always due to liver disease. Also check for gynaecomastia and alopecia, both of which can result from increased oestrogen levels.
Begin by inspecting the abdomen for the following features:
Abdominal distension: This is usually due to one of the six f's; fat, foetus, flatus, faeces, fluid or fulminant tumours.
Caput medusae: This describes tortuous veins surrounding the umbilicus. Its presence suggests porto-systemic hypertension due to liver pathology.
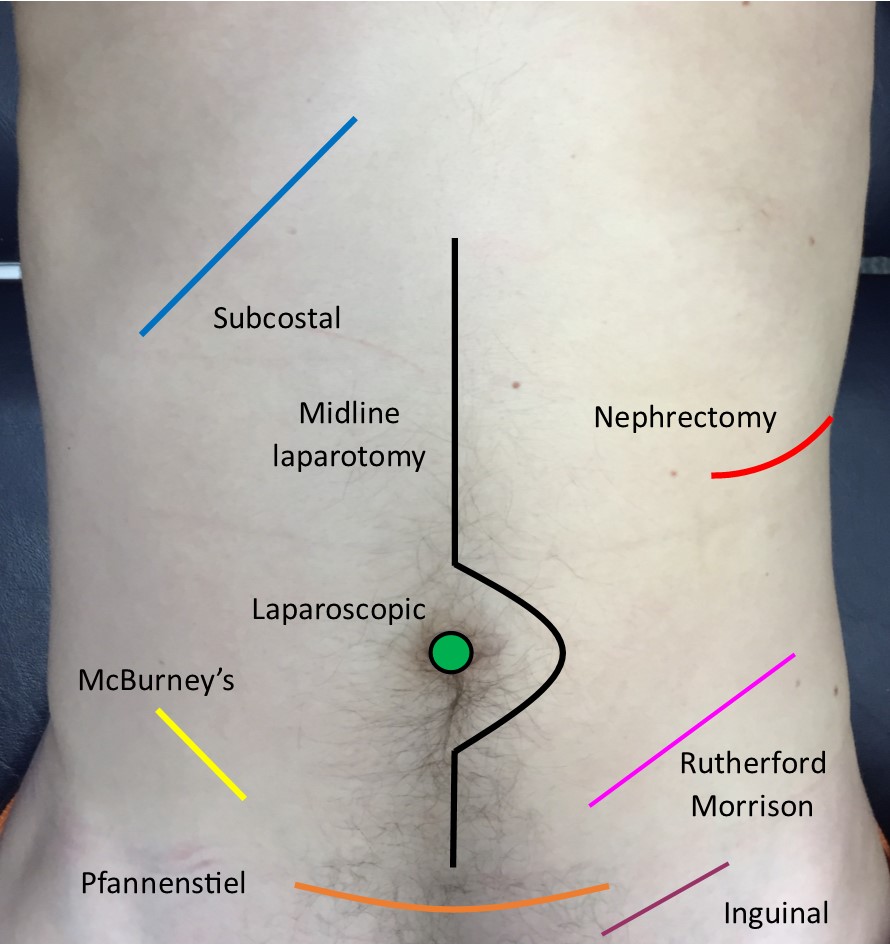
Scars: There are a number of important scars to be aware of. Examples include subcostal/Kocher's (cholecystectomy), midline (laparotomy), nephrectomy (renal surgery), McBurney's or Gridiron's (appendectomy), umbilical laparoscopic (resection), Pfannenstiel (hysterectomy), inguinal (hernia) and Rutherford Morrison (renal transplant) scars.
Stomas: A stoma is an external bag in which faeces is deposited as a result of an interruption to the alimentary canal due to previous surgery.
Cullen's sign (central grey/purple tinge to the skin) or Gray-Turner's sign (tinge in the flanks): These alarming signs suggests haemorrhagic pancreatitis.
Striae (stretch marks): Usually suggests Cushing's syndrome. However, profound weight loss (e.g. due to cancer), ascites or pregnancy can all result in striae.
Common abdominal scars.
Palpation
Before palpation, lie the patient flat on the bed, and once again ask if there is any pain.
Lightly palpate the nine abdominal regions whilst making sure to observe the patient's face for any reactions. If the patient mentions any pain, begin palpation at the region furthest away from the pain, and then aim to localise the centre of the pain.
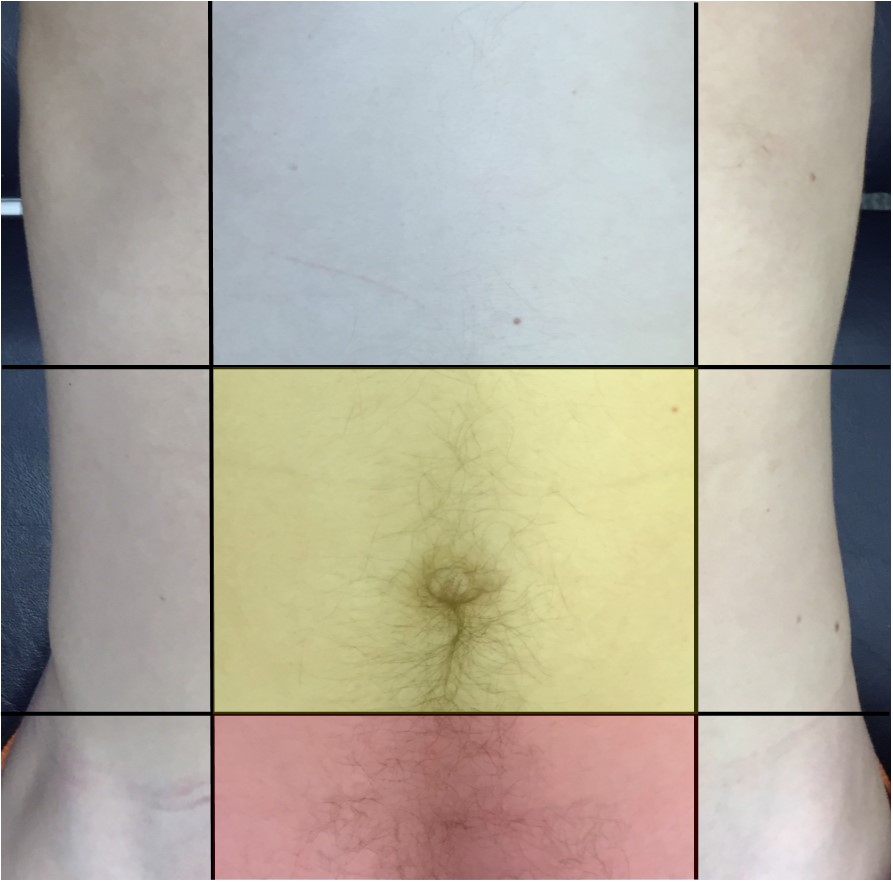
The nine abdominal regions.
Also check to see if the pain is on palpation or release. Peritonitis presents with what is known as rebound tenderness, a phenomenon where the pain is greater on release. If the pain is located in the right iliac fossa you can check for Rovsing's sign. This is a phenomenon where medial pressure in the left iliac fossa produces pain in the right iliac fossa, and is indicative of appendicitis.
Follow up with deep palpation, this time with the intention of feeling for any masses. Use one hand on top of the other for additional support and control.
A good tip during palpation is to crouch to the same level of the patient. For tall individuals, this may involve getting down to your knees.
The epigastric (blue), umbilical (yellow) and hypogastric (red) quadrants are highlighted in the image above. These are important as pain from the foregut, midgut and hindgut is respectively referred to these quadrants.
Patients with peritonitis may present with tense abdominal wall muscles. This is known as guarding, and can make the examination more difficult. In these cases, do your best to help the patient relax.
Next palpate the abdominal organs in turn.
Liver
Palpate just superior to the patient's right anterior superior iliac spine and palpate systematically upwards, asking the patient to inhale and exhale each time. As you approach the costal margin, the liver should eventually become palpable on inspiration. If enlarged, note the enlargement in centimetres from the costal margin. The gallbladder may also be palpable.
If there is any pain then attempt to elicit Murphy's sign. This is done by asking the patient to inspire as you palpate underneath the free-edge of the liver. If the patient suddenly stops their inspiratory effort due to pain, then this is indicative of cholecystitis.
Hepatomegaly may be due to a malignancy, hepatitis, or in the context of result of right ventricular failure (nutmeg liver).
In the case of jaundice, if the gallbladder is palpable but there is no pain, then, per Courvoisier's law, the cause of jaundice will not be gallstones. This is because gallstones will cause chronic inflammation which results in scarring of the gallbladder, and therefore it will not be palpable as the scarring prevents expansion. In such cases, pancreatic cancer or perhaps a mucocele obstructing biliary flow is a more likely cause of the jaundice.
Spleen
Palpating the spleen occurs in similar fashion; begin at the patient's right anterior superior iliac spine, and palpate systematically up and diagonally left across the patient's abdomen. On approaching the left costal margin, the spleen is eventually palpated on inspiration. The spleen may be enlarged due to portal hypertension.
Kidneys
Placing one hand 2cms lateral to the spine on the patient's back. Place the other hand anteriorly in the corresponding flank. Push into the patient's back to "ballot" the kidney and repeat on the other flank. If there is an enlarged kidney, it will become palpable on the anterior surface of the patient. The kidneys are not usually palpable in healthy patients unless they are very thin.
Bladder
The bladder can be palpated in the suprapubic area. Start at the umbilicus and palpate downwards to the pubis bone. Do communicate with the patient first however, as palpation can be very uncomfortable on a full bladder.
Aorta
Using two hands, palpate the midline superior to the umbilicus. If the hands diverge with each pulsation, an abdominal aortic aneurysm may be present.
An aortic aneurysm is a permanent localised dilatation of the aorta to greater than 150% of its normal diameter.
Percussion
Percuss the liver and spleen in the same pattern as used in palpation (described above). The bladder can also be percussed by starting in the umbilical region, and percussing downwards until there is a change in note (dullness). This may be more difficult if the patient has an empty bladder.
You should also percuss for ascites. Start at the umbilicus and percuss laterally to the patient's left-hand side. A dull note may be heard as a result of fluid pooled laterally by gravity. Keeping the fingers over the area of dullness, ask the patient to lay down on their right-hand side, and after 30 seconds, check if the note becomes resonant. If this is the case, then this is termed shifting dullness and suggests ascites.
Auscultation
Auscultate over two places on the abdomen for bowel sounds. Absent bowel sounds over a period of three minutes can be a sign of ileus (failure of peristalsis) or paralysis. In an OSCE environment however, simply listen for 10 seconds. Tinkling bowel sounds are a sign of bowel obstruction. Finally, a bruit over the liver can indicate hepatocellular carcinoma.
You can also auscultate over the area of the renal arteries for bruits due to renal artery stenosis. However, this may be difficult to hear.
Ankles
Check the patient's ankles for pitting oedema which may present if the patient has hypoalbuminaemia.
Completion
Complete the examination by offering to palpate for an inguinal hernia, examine the external genitalia and conduct a digital rectal examination. You're examining the external genitalia to look for varioceles in males. The left spermatic vein drains into the left renal vein, whereas the right spermatic vein drains into the inferior vena cava. Therefore, a left variocele may indicate a retroperitoneal mass, such as a renal cell carcinoma or polycystic kidney disease.
Key
Headings - items highlighted in green are important headings to cover.
Definitions
Stigmata - a clinical sign relating to a particular condition. E.g. clubbing and infective endocarditis.
Paraphenalia - equipment the patient may have by the bedside.
Presentation
Thank you for allowing me to conduct an abdominal examination on [patient's name], a [age] year old [male/female]. On general inspection, there were no paraphenalia around the bed, and the patient appeared comfortable and well at rest. On examination of the hands, there were no stigmata to suggest disease. Asterixis was not elicited. There were no excoriations or unexplained bruises on the arms. The pulse was regular at [x beats per minute]. I would like to formally assess blood pressure. On examination of the head, there was no conjuctival pallor or icterus. In addition, there were no stigmata of disease in the mouth. In the neck, virchow's node was not enlarged.
On closer inspection of the abdomen, there were no drain sites, stomas or scars to suggest previous surgery. On palpation, the abdomen was soft and non-tender, with no organomegaly. The abdominal aorta was non-expansile. Bowel sounds were present and normal. Finally, there was no peripheral oedema. To conclude, this was a normal abdominal examination .
Interactive markscheme
When assessing each other, click on each list item as you go along. Doing so will turn the list item green. Make careful note of any steps missed at the end.
We recommend completing any examination or procedure in under 10 minutes, but you can adjust the timer to suit your needs.
:
Introduction: “Hello, I’m SimpleOSCE and I am a medical student. I need to examine your tummy/abdomen today, would that be okay? Can I confirm your name and DOB? Thank you.”
"For the purpose of this examination the examiner will act as a chaperone."
Wash hands.
Position the bed at a 45° angle and ensure adequate exposure.
Ask about pain and discomfort.
Check for incisional hernias.
Inspect the patient (skin colour) and their surroundings (stoma bag).
Inspect the hands for clubbing, koilonychia, leukonychia, palmar erythema and Dupuytren's contracture. Inspect the arms for excoriations.
Take the pulse while assessing for liver flap (ideally for 30s).
Offer to measure the patient's blood pressure.
Examine the eyes for jaundice, anaemia and Kayser–Fleischer rings.
Examine the mouth for ulceration, glossitis and angular stomatitis.
Inspect the upper chest for spider naevi and gynaecomastia.
Inspect the abdomen for distension, caput medusae, scars and striae.
Lie the bed flat.
Palpate the 9 regions superficially and then deep.
Look at patient's eyes during palpation and ask them to report pain.
Palpate for the liver and spleen.
Ballot the kidneys.
Palpate the bladder and for an abdominal aortic aneurysm.
Percuss the borders of the spleen, liver and bladder.
Percuss for ascites by assessing shifting dullness.
Auscultate in 2 places for bowel sounds (paraumbilical) and for renal bruits.
Palpate the legs for peripheral oedema.
Thank and re-cover the patient.
“To conclude I would like to take a full history, check for any herniation, examine the external genitalia, perform a digital rectal examination and dipstick the urine”.