Introduce yourself, confirm the patient's name and date of birth, obtain consent and proceed to wash hands.
Ask the patient to remove any dentures and to sit on a chair and face you. Check if they are in any pain or discomfort and offer analgesia if necessary.
Patients with severe odynophagia (pain on swallowing) are more likely to suffer from trismus (reduced opening of the jaw, also known as “lockjaw”). This can greatly hinder your ability to examine and therefore it may be appropriate to offer analgesia and examine the patient after this has taken effect.
Equipment
Collect the following equipment:
Head torch: If you are unable to obtain one of these, a pen torch is a suitable alternative. The advantage of a head torch is that you are able to manoeuvre your light source to your liking whilst keeping your hands free to examine.
2 tongue depressors: This may be metal or wooden. Wooden tongue depressors are cheap and disposable.
A pair of non-sterile gloves.
Clinical waste bin.
Inspection
General inspection
Start by facing the patient and observing for any obvious swelling around the cheek or mandible, which may be due to swollen parotid or submandibular glands.
In addition to multiple small salivary glands littered around the mucosa of the oral cavity there are three large salivary glands which open into it on each side:
Parotid gland: The largest of these, parotid gland sits outside of the cavity just superior to the angle of the mandible. The parotid duct emerges into the oral cavity just adjacent to the crown of the second upper molar.
Submandibular gland: The majority of the submandibular gland (“superficial” part) sits inferior to the mylohyoid muscle and is just outside of the oral cavity. Its “deep” part extends over the muscle and lies on the floor of the cavity. The submandibular duct opens just beside the base of the frenulum of the tongue.
Sublingual gland: The small, sublingual gland sits on the medial aspect of the mandible at its most anterior part, just lateral to the midline, lying entirely on the floor of the oral cavity. As such, it drains into the cavity itself via multiple small ducts.
General causes of salivary gland enlargement include:
Sialolithiasis: The presence of a calcified salivary stone (sialolith) usually in the duct of a salivary gland. Wharton’s (submandibular) duct is most commonly affected.
Sialoadenitis: Infection of a salivary gland, often secondary to sialolithiasis. Most commonly the cause is Staphylococcus aureus, however other causes include viral agents such as HIV and herpes simplex virus. Mumps is especially well known to cause parotid gland sialoadenitis (parotitis).
Tumours: There are a vast number of neoplasms which can occur in the salivary glands. These range from benign causes such as pleomorphic adenoma to malignant carcinomas and adenocarcinomas.
Unique causes of parotid enlargement include:
Sjogren’s syndrome: Lymphocytic infiltration of exocrine glands, resulting in xerophthalmia (dry eyes), xerostomia (dry mouth) and enlargement of the parotid glands.
Sarcoidosis: This is almost always bilateral and is due to granulomatous infiltration.
Alcoholism: For unknown reasons, alcoholism can cause chronic swelling of the parotid glands
Ask the patient to open their mouth and use your torch to inspect the patients lips for any colour changes, such as “brown freckles” found in Peutz-Jegher’s syndrome, or signs of inflammation (stomatitis/cheilitis). Look for any ulcers (sores) which may be sequelae of erythema multiforme or infections, such as syphilis or herpes simplex virus. Very rarely, a lip ulcer with a hard edge may be due to cancer.
Briefly observe for inflammatory dental disease in the gums (gingivitis) and teeth (periodontitis).
Hereditary intestinal polyposis syndrome, or “Peutz-Jegher's syndrome,” is an autosomal dominant disease characterised by the development of benign hamartomatous polyps in the gastrointestinal tract and hyperpigmented macules (brown freckles) on the lips and oral mucosa.
Inflammation of the mouth and lips (stomatitis) or the lips only (cheilitis), is most commonly caused by irritation at the corners of the mouth (called angular cheilitis). This can be precipitated by vitamin (B2) and mineral (iron) deficiencies or candida infection.
Ask the patient to stick out their tongue and move it from side to side to observe for any obstruction, which may be due to swellings.
Inspect the tongue for:
Macroglossia (large tongue): This can be caused by a variety of congenital and acquired conditions, such as vitamin B12 deficiency.
Glossitis (inflammation of the tongue): There are multiple causes of glossitis including vitamin (B) and mineral (iron) deficiencies, infection, Crohn’s disease, oral lichen planus and many more. Types include atrophic glossitis and strawberry tongue.
White patches: Multiple widespread white patches are usually a result of a Candida albicans infection and can occur in HIV infected patients or those with diabetes mellitus. Rare causes include hairy leukoplakia, a sequela of Epstein-Barr virus found in infected immunocompromised patients and linea alba, a thin white line of benign nature.
If there is any abnormal tongue movement, perform a cranial nerve examination.
Glossitis refers of inflammation of the tongue. This can be infective or nutritional in origin. The tongue will be sore, the dorsal surface will usually be smooth and erythematous, and there will be absence of some of the lingual papillae. Two important types of glossitis are as follows:
Atrophic glossitis: A depapillated, glossy and tender tongue usually caused by an iron deficiency anaemia or due to a vitamin B12 deficiency.
Strawberry tongue: An erythematous tongue with relatively enlarged fungiform papillae. Causes include scarlet fever and Kawasaki disease.
Use your tongue depressors to manipulate the tongue and have a good look at the buccal mucosa. Ask the patient to lift their tongue to view the floor of the oral cavity and then to tilt their head back so you can observe the hard palate.
Identify any:
Aphthous ulcers (round, shallow ulcers confined to the mucosa of the mouth): These may occur in coeliac disease, inflammatory bowel diseases, erythema multiforme or be secondary to a herpes simplex virus infection.
White patches: Again, due to Candida or leukoplakia.
Submandibular duct stone: A salivary stone (sialolith) causing blockage of a submandibular duct.
Sublingual/submandibular gland swelling: This may be due to a variety of causes of salivary gland disease, such as sialolithiasis, sialoadenitis, Sjogren’s syndrome or neoplasm.
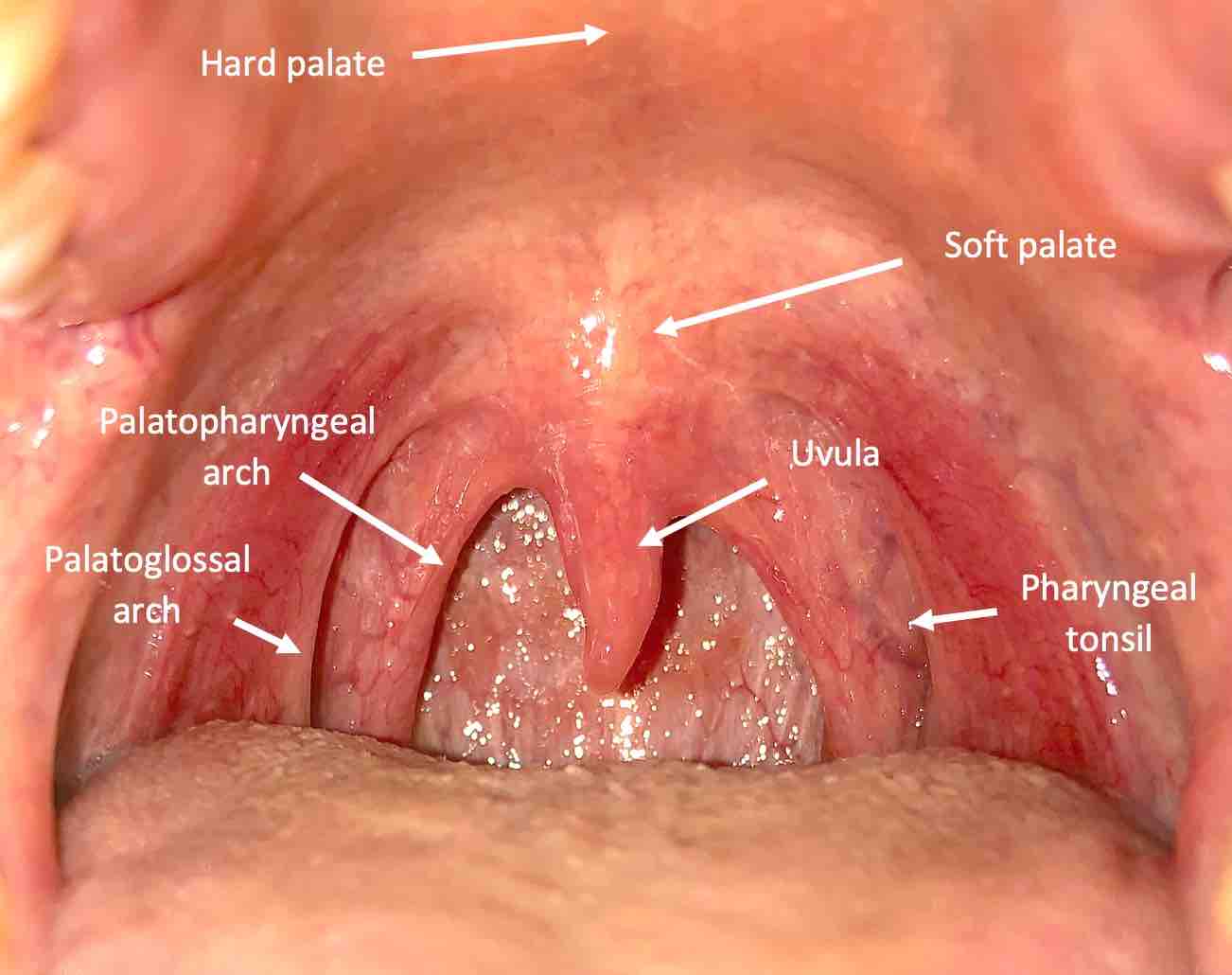
Ask the patient to centre their tongue. Using your tongue depressors, gently press the tongue so that you can get a good view of the oropharynx. Identify the soft palate and uvula. Mucosal changes described above may also be present here. Position your torch to get good views of the anterior palatoglossal and posterior palatopharyngeal arches. The pharyngeal tonsils will be sat in the tonsillar depressions in between the pharyngeal folds (pillars) which form the arches.
Palpation
Identify the various structures in the oropharynx.
Inflammation of the pharyngeal folds and uvula will be present in pharyngitis. Pharyngitis may also present with uvular swelling. Other causes of swelling include injury (for example, during intubation) or acid reflux.
Identify the position of the uvula. Deviation with the absence of any other signs or symptoms may be normal, but otherwise may be due to a contralateral glossopharyngeal nerve lesion (the uvula is deviated “away” from the lesion). If there is nearby palatine swelling, such the presence of a peritonsillar abscess (quinsy), then this will push the uvula to the contralateral side.
In most healthy individuals, the tonsils can be difficult to identify. Chronic, bilaterally enlarged tonsils are usually benign. Causes of a unilateral tonsillar enlargement however include papilloma and carcinoma. Pharyngitis may spread to the tonsils causing tonsillar inflammation (tonsillitis). Swelling is often bilateral, usually with one tonsil swelling more than the other. White exudate may be present if the cause is bacterial in nature.
Tonsils will be absent in a tonsillectomy; white granulation tissue is often present in the weeks immediately following one.
Asking the patient to say “aaah” will cause them to naturally depress the base of the tongue and aid you in your examination.
Inflammation of the pharynx is known as pharyngitis. The patient will present with odynophagia and fever. This is typically caused by “common-cold” viruses such as adenovirus and are self-limiting. More aggressive viruses include Epstein-Barr virus and measles virus. Bacterial infections are much less common but are almost always due to Group A streptococcal species such as Streptococcus pyogenes.
Tonsillitis is a subtype of pharyngitis, and hence has the same aetiology and presentation. Both viral and bacterial tonsillitis can cause swelling, but only the latter presents with exudate. Numerous infections of tonsillitis requiring antibiotics (>7 in the span of a year) may warrant consideration of a tonsillectomy.
One of the complications of bacterial tonsillitis is infection spreading to the peritonsillar space forming a peritonsillar abscess, also known as a “quinsy.” An untreated peritonsillar abscess can lead to oropharyngeal obstruction and trismus (due to odynophagia). The size of the tonsils has no bearing on the presence or absence of a peritonsillar abscess; often the complication occurs when the tonsils are barely enlarged.
Put on the non-sterile gloves. Ask the patient if they mind if you palpate around the oral cavity.
Bimanually palpate the floor of the oral cavity, identifying any sialoliths or swelling of the submandibular or sublingual glands. Next palpate the lateral wall for swelling of the parotid gland. Characterise any such swellings assessing for size, tenderness, texture and consistency.
Use your index or middle finger to palpate on the inside of the oral cavity, and your thumb or a finger of the opposing hand to palpate externally. You may choose to do this with one or two hands depending on their size.
Completion
Complete the examination by thanking the patient, disposing of equipment and washing your hands. If appropriate, offer to examine the ears, nose, neck and cranial nerves. Further investigations would warrant referral to any of the following teams, depending on the pathology identified:
Ears, nose and throat.
Head and neck.
Dental.
Present and/or document your findings.
Interactive markscheme
When assessing each other, click on each list item as you go along. Doing so will turn the list item green. Make careful note of any steps missed at the end. We recommend completing any examination or procedure in under 10 minutes, but you can adjust the timer to suit your needs.
:
Introduction: "Hello, I'm SimpleOSCE and I am a medical student. I've been asked to examine your mouth and throat today. Can I confirm your name and DOB? Thank you."
Explain examination and obtain consent: “This will involve me using a torch to look inside the mouth. I will be using some tongue depressors to which may be a little uncomfortable, so let me know if you are in any pain.”
Wash your hands.
Check if the patient is in pain or discomfort. Use analgesia if necessary.
Assemble the correct equipment including a torch, 2 tongue depressors and a pair of non-sterile gloves.
Inspect for any obvious parotid or submandibular swelling.
Ask the patient to open their mouth and inspect the lips for colour changes (such as brown freckles), inflammation (cheilitis) and ulcers.
Inspect the gums and teeth for dental disease.
Ask the patient to stick out their tongue and move it from side to side.
Inspect the tongue for macroglossia, glossitis and white patches (candidiasis).
Inspect the buccal mucosa, cavity floor and hard palate for aphthous ulcers, white patches, submandibular duct stones and sublingual/submandibular gland swelling.
Throughout the examination, use your tongue depressor to obtain a better view.
Identify the pharyngeal folds and uvula for inflammation and swelling and the tonsils if they are enlarged.
Put on non-sterile gloves.
Palpate the floor and wall of the oral cavity looking for any sialoliths or salivary gland swelling.